In Global Peace Through The Global University System
2003 Ed. by T. Varis, T. Utsumi, and W. R. Klemm
University of Tampere, Hameenlinna, Finland
ALTERNATIVES IN "E-LEARNING"
FOR HEALTH PROFESSIONALS
IN LATIN AMERICA AND THE CARIBBEAN
Pablo A. Pulido M.
Pan American Federation of Associations of Medical Schools
and
Jaime Requena
Fundacion Universidad Metropolitana
Introduction and Raison D'Ítre
Initially, distance education mostly involved the distribution of printed material. Later, visual aids were added to complement its potential. This kind of model did not permit ample interaction between learners and teachers, which is a fundamental value of traditional classroom education. Developments in recent years include cable or satellite-based electronic networks to facilitate a low cost and geographically extended data transmission. Cable and satellite are thoroughly changing teaching methodology in distance education, transforming it into an alternative that competes with classical teaching methods by incorporating a real-time interaction component. New digital technologies offer the added advantage of specifically aiming the programs to those who are being taught, either at their workplace or their homes, when they so require.
On the other hand, a dramatic increase of demand for knowledge and the application of social justice impose an urgent need to improve effectiveness in the supply of Public Social Security and Health has triggered in Venezuela, as in many other countries of the region, a meticulous process of reforms that must be assessed for efficacy. An orderly process of decentralization of services should place resources and management within reach, so that end-users may appraise their quality and correspondingly demand any relevant improvements. The goals are to attain more effectiveness at the least cost possible and to implement health policies that lead to real improvement in quality of life, both paradigmatic of the reform models.
Training, progressive qualification and robust education are of utmost importance in these paradigms. The overall purpose is to offer quality training and continuous education and development, in classrooms or extra-mural, interactive with human, professional and technical resources working in the most critical areas of management, planning, organization and provision of health services through the use of real time methodologies and new IT means applied to the control of communication and education sciences.
For Whom? Source of Demand
There is a double source of demand for services: institutional and personal. Initially, the demand will basically arise from the public education system of health professionals and technicians. In this initial phase, recipients of information and courses will be of two kinds: technical staff of health divisions or institutions in every state, and managing, medical and nursing staff of hospitals and ambulatories in the individual states. Later, or even simultaneously, courses should be aimed at both demand segments (institutional and personal) including the Schools of Medicine and Departments of Health Sciences in the university sector, as well as the community. Course content will encompass the most common medical specialties, review of relevant pathologies, and familiarization with effective managing, behavioral and technical procedures according to the demand of the population to be served.
Political Basis
In Venezuela, as in all countries of Latin America, the State is obliged by constitutional mandate to guarantee health of the people. Therefore, it must develop programs and actions in order to honor this citizen right. Health is a process determined by multiple and complex factors, among them, a diversity of economic, social and environmental conditions; access to, coverage by and quality of health services and level of education of the population in general and particularly health service providers. Consequently, training and review courses for health service personnel are a key factor in complying with the constitutional and institutional objective of securing a better quality of life for the people. Thus, we have the urgent need to improve efficacy in the provision of health services by sponsoring a thorough process of reform in the public system of health and social security. This requires, as a first step, a reformulation and implementation of a more efficient health education system.
New relationships among health service providers, regulating agencies and the population at large must be established, the most important being the one directly related to the users, that is, between the state and municipal agency responsible for the provision of services and the health institutions where such services are provided. Therefore, the proposed move of resources and their management toward users of the service will enhance their ability to appraise quality and demand any pertinent improvements. More effectiveness at the least cost possible is the basic requirement of such reform. Now, in view of institutional frailties of the system, particularly upon the enactment of new legislation or under high impact conditions such as endemic diseases or occasional contingencies, training and education are imperative.
Technological Basis
Dynamic development of low cost and long range cable- or satellite-based data transmission electronic networks and corresponding day-to-day IT innovations have radically changed the teaching methodology of extra-mural education by incorporating a real-time interaction component. As a result, efficacy and efficiency have drastically improved, and the methodology is today a valid alternative to traditional teaching methods. Also, a significant expansion of the access and distribution systems by the telephone and communications industry has resulted in a regional exponential growth of Internet users to a total of around three million in Venezuela. A combination in a crossed platform of both technologies, emission of digital TV signals and Internet, with the support of conventional teaching systems permits the delivery to the most remote places of multimedia interactive distance education programs designed to meet the training and education needs of modern professionals. Providing fast transmission speeds for excellent quality images (indispensable for telemedicine processes), the digitalization of TV signals permits the use of Internet via either IP protocols or satellite systems (DirecTV or similar). New digital technologies confer an added advantage to extra-mural education by permitting students to receive specific training programs when needed, either at work or at home. It is worth mentioning that the methodologies required for an effective use of these new teaching systems are very specific and significantly different from traditional education techniques. Medical doctors and other health professionals in the country have dire needs in terms of medical evidence (primary information), continuous education and health services. Therefore we must implement mechanisms that will meet those needs.
Relevant Contents
There are not many national or regional organizations capable of offering the necessary content and quality required by health professionals. Examples include the FEPAFEM / PAFAMS, the Pan American Federation of Schools of Medicine Associations, and affiliates. Today, most of the existing operations are commercial and oriented to consumers rather than to health professionals and technicians. Some Schools of Medicine in the region, mainly those in Brazil with the current addition of Peru, Mexico and Colombia, are trying to offer distance education programs, mostly aimed at their own undergraduate and graduate medical students. Cost limitations generally hinder access to state-of-the-art technologies. Lastly, there is a disturbing tendency towards the creation of self-medication sites inadequately monitored by good and relevant medical practice institutions. We believe that the Schools of Medicine of the continent, along with those of Brazil, Argentina, Chile, Colombia, Peru, Mexico and particularly Venezuela could make very important contributions, especially if they are consistent with changes demanded by society.
On the other hand, new health disciplines are likewise developing to the point that other health professionals today perform many of the tasks traditionally accomplished by physicians. Such changes impose on health professionals and technicians the need for a continuous knowledge upgrade. However, well-trained professionals who therefore require continuous training to remain updated in technological breakthroughs must necessarily perform health activities. The new medical, managerial and information technologies require more and better-trained professionals. Consequently, the areas of education and professional practice monitoring are key for the success of new health policies; unfortunately those are the areas receiving less attention.
Medical knowledge is doubled every three to five years. Duly certified specialization accompanied by institutional accreditation, rapid medical advances, and changes in health systems likewise generate the necessary redefinition of traditional forms of practice.
In brief, since the paradigm on which reform processes are based is services of higher quality and efficacy at the least cost possible, education and training is required particularly with regard to the systems institutional weakness.
Generating Coherent Action Projects
Preliminary Approach and Evolution
In 1998-99, the Interamerican Development Bank (IDB) started the Initiative known as "Informatics 2000" with the purpose of sponsoring a display of novel high technology communications and informatics initiatives in the public and private sectors by the year 2000, with particular emphasis in those representing factors of economic growth and social development in Latin America and the Caribbean. Thus, at a meeting of Heads of State and Government in Santiago de Chile on April 1998, a panel of experts and scientists that cooperated in the process of the Initiative "Informatics 2000", identified the kind of technological infrastructure that should be supported and indicated the characteristics of policies and institutional developments required, in the assumption that Internet would be crucial and fundamental for the process.
[Several additional events included the Conference "Telecommunications in Health and Health Care" sponsored by OPS/PAHO and the KOOP Foundation. The Preparatory Meeting for the project INFORMATICS 2000, convened in Washington D.C. An experts meeting on the role and options to apply Telecommunications to Health Systems in Latin America and the Caribbean, took place in 1997. The "First Annual Telemedicine / TeleHealth Conference" INTERCOM, that was organized in Miami. The Preparatory Meeting of the working group in health issues for the Initiative INFORMATICS 2000 for Latin America and the Caribbean was sponsored by the Interamerican Development Bank and the Pan American Health Office and held in 1997. The Conference "II Latin American and Caribbean Meeting" of the Working Group in Health Issues for the Initiative INFORMATICS 2000 met in Mexico City (1997) under the auspices of the IDB and PAHO.]
The presentation of the Venezuela Case outlines the guidelines for a Virtual Education in Health Sciences for Latin America and the Caribbean through the project Vi@Salud, an initiative of FEPAFEM-PAFAMS. This decision resulted from conferences such as "III Latin American and Caribbean Meeting" and the informal meeting of the Working Group in Health Issues for the Initiative INFORMATICS 2000. Likewise, the issue was subject of presentations at the XVI Pan American Conference of Medical Education, sponsored by FEPAFEM and convened for Buenos Aires in November 2001. Through the Initiative INFORMATICS 2000, the IDB expressed its commitment of working together with the regional Ministries of Health, PAHO and CITEL (the authority in regional telecommunications).
Non-government organizations, among them FEPAFEM, and a number of high-tech corporations that include the pharmaceutical sector, are currently oriented toward the development of projects. Specifically, the working group in health issues, formed by regional experts, the Pan American Health Office and the World Health Organization (WHO), though without a firm funding commitment, recommended the following programmatic elements:
- A web site for issues of medical and health information.
- A continuous education regional program, under the auspices of FEPAFEM, on the virtual environment for professionals of the health sector.
- Develop application packages or groups (including funding) for small health units.
- Develop service packages and communications & informatics equipment for health networks, including the tools required for improving productivity and efficiency.
General and Specific Objectives of the "Project FEPAFEM -- Vi@Salud"
The project's general objective is to provide quality continuous education of a virtual or extra-mural nature to human resources, professionals and technicians, working in the most critical areas of health services management, planning, organization and provision, through the use of real time interactive teaching methodologies developed for communications and informatics disciplines. The specific objectives are to:
a) Significantly improve the institutional management of ambulatories and hospitals;
b) Improve performance of professionals and technicians by keeping evidence-based high quality updated information;
c) Improve relations with the community through interaction with the health team by stimulating their active participation in the appraisal of services provided with a view to a healthy quality-based institutional and programmatic accreditation;
d) Develop a high level of satisfaction among users of the health sector with regard to services provided and received.
Methodologies and Alternatives for Achieving the Objectives
The model uses new education technologies while adapting certain traditional technologies typical of classroom systems (use of printed material, libraries and CD-ROMs) that will be reinforced by the use of virtual mechanisms. The project is based on technologies that ensure a greater potential impact than those used in the traditional system. These new technologies do not imply that the student will abandon the search of scientific or information material through other means. On the contrary, it promotes and encourages even higher levels of use than those attained with traditional systems in view of the abundant resources available in the Web -- the largest library of mankind -- and its powerful specialized search engines. Vi@Salud faces two great challenges: pedagogical, given by the nature of the teaching method, the quality of contents and degree of teacher-student interaction; and technological performance, given by the hardware required for transmission and reception of courses, which in the end is of lesser importance. The Vi@Salud project is based on the so-called "paradigm of virtual education."
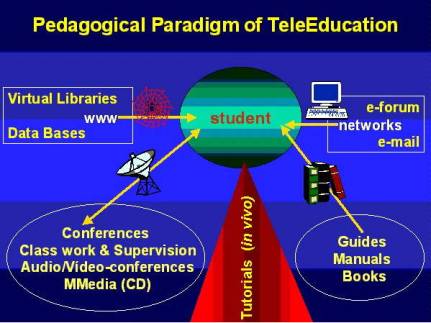
Figure 1: Pedagogical Paradigm of TeleEducation
It could be represented by a triangle where the base is Publications and Prints, followed upwardly by the Web to finally end in the vertex by the TV Component. The student starts watching television (intentional education), then goes to the Web (incidental education), and receives graphic material, printed copies, the study guide and tests (similar to a folder received when attending a several days course) and finds search engines for linking to virtual libraries and other web sites. Finally, the student will also have available for personal use, a book or CD (base of the triangle). The project's strategy is based on the utilization of Internet broadband communication facilities, specifically those characteristic of television media, for the development of courses adapted to the training needs of human resources in primary health care level (ambulatories) and secondary health care level (hospitals). Once Internet channels are opened, facilitating an easy TV signals transmission, the possibilities of courses offered is almost unlimited, the sole restrictions would be preparation capabilities and facilities to adapt those made in foreign countries.
Therefore, the initial environment for community medicine and first stage of nursing followed after their respective evaluations by the second stage, could gradually extend to incorporate a number of other fields and specialties: dentistry, pharmacy, and health management and funding. Likewise, the strategy permits streamlining of very specific courses with a high social content, for instance those aimed at indigenous communities that would be prepared in their native language. The plan involves starting the teaching component with an intensive use of Internet and all other multimedia advantages, including videos whenever possible either by mailing pre-recorded tapes (initial stage) or by their TV distribution via broadband Internet (second stage). In any event, the model adopted does not consider (or minimizes) the use of live TV broadcasts (teleconferences) but rather favors pre-recorded presentations.
Two reasons support the modality chosen: first, reuse of pre-recorded videotapes will maximize return on a very high initial investment, since preparation in television studios of high academic and technical quality pre-recorded courses is very expensive. In addition, the useful life of a course is estimated in five years with up to four broadcasts per year. Second, the pre-recording method helps to eliminate teaching uncertainties caused by improvisations, a common problem in the case of conferences. Distance education courses, by definition, must observe clear academic objectives only attainable by full compliance of a schedule. In view of the fact that the teaching model to be adopted will modulate the nature of technology operation components, it is imperative to define the technology components at the Training Centers, where students will receive their courses, and at the Control and Administration Center, where the interactive teaching components where tutorial follow-up and evaluation originates.
Figure 2: Scheme of Operation of Vi@Salud
Control Center and Training Centers (individual work stations) will be connected via Internet and WWW. The Control Center will be located in Caracas and connected to FEPAFEM headquarters, where a good part of the network is already in place. The Center must have capacity for administering paid services and databases and should have restricted access and protection systems. Installation and maintenance costs of four pilot training centers, as well as their location and nature, will be covered with funds given by the State or by its own users. Initially, training centers would be housed in pilot hospitals, ambulatories or other sites indicated by the training recipient agency, among which the COMMUNITY INFOCENTERS currently under development. Individual subscribers only need equipment similar to a computer workstation in a training center; these centers would have several PCs in a network with multimedia capacity and full broadband access to Internet.
In the beginning, a videotape recorder would be required for pre-recorded tapes and eventually, it might be necessary to install a system with capacity for processing satellite video signals, like Telemedicine. Later, in more advanced stages, consideration could be given to the use of a TV-signal decoder whose cost would depend on the system chosen for the TV-signal. At present, users can be reached at their workplace or their homes with text, data, sound and image via four different electronic platforms for independent or joint use:
- Internet,
- Analog television,
- Digital and satellite television, and
- Television via Internet (IP) on the PC.
These four systems are presently converging, and experts seem to agree that either the 3rd or the 4th option will control the market with an integrated high interactivity platform via high speed modems (like ADSL in the telephone company's network).
Today, distribution of open TV signals in Internet is a reality, limited only by the CPU's processing speed and the access lines to Internet (modem or broadband). With new processors and improvements in data transmission protocols, it is expected that in the near future TV and PC will converge on a single technological platform. Thus, projects like Vi@Salud will no longer require the assistance of conventional or satellite TV-signal carriers and distributors. On the contrary, they will be able to place their TV-signal in Internet at a minimum cost. As a counterpart, signal recipients --public institutions and private subscribers- will require the most advanced computers equipped with last generation processors and modems.
The problem is far more complex with regard to satellite TV because of the video decoder required. Options change dynamically, as in a system like DirecTV or satellite decoders like IMPSAT (or using the IP protocol to carry the signal in Internet, as explained above). In the first case, the decoder is part of a commercial package and the equipment requirements for receiving the satellite signal are minimal. Individuals can hardly set up the infrastructure required for receiving TV satellite signals, and it could only be justified for a conglomerate of recipients (for instance, a corporation or educational institutions like the Technological Institute for Higher Studies, ITESM, in Monterrey, among others).
Expected Impacts
There is no doubt that a
Global Informatics Society will render great benefits. However, to enjoy those
benefits full and global access to Internet is required and even if this were a
reality for all, there are many side issues to be considered, for instance,
contents, intellectual property, security, privacy, quality and human
resources. There are six evident potential benefits:
- Improving integral health care for the less privileged.
- Fostering a more democratic, participative, open and competitive society.
- Offering the best possibilities of professional growth and capability enhancement to health professionals practicing in remote places devoid of educational support.
- Encouraging a low cost use of technologies and mechanisms for accessing systems developed by the revolution in informatics --Web and Internet-- and those that should exist in the so-called community centers or INFOCENTERS, guaranteeing access to all but mostly to those in remote and isolated regions.
- Sponsoring the formation of a "backbone" or broad range regional communication system that could be used by the public and private sectors and society in general, including the military.
- Approving public policies that justly and transparently allow society to take on the range of services and technologies seen as more reasonable and necessary for the citizenry, particularly in those cases where the market forces cannot encourage alone the necessary incentives for the less privileged to actually receive the expected benefits, in keeping with the overall objective of achieving equity and enforcement of ethical principles.
Transfer of Results
Once these experiences are developed and appraised, they will constitute a firm reference for the implementation of a Professional and Technical Continuous Education process with real national and regional coverage that will benefit all users --staff and patients-- of health services. Further, beyond our national borders, a project so beneficial should be taken up as a model by other Spanish-speaking nations of the region. All educational processes and courses developed in Venezuela during the first stages of the Pilot Project will be shared with those countries that request it, on the basis of agreements, in order to warrant success of the project and favor a transfer of technology indispensable for creating a process of accreditation and new certification of professionals and technicians, required by globalization in economy and telecommunications.
With respect to users or petitioners of process results, data of human resources in the health sector must be updated. For instance, the list of health professionals in Venezuela is as follows: 53,818 physicians, 8,571 pharmacists, 13,000 dentists and 14,676 certified nurses. Almost all countries of the region have surpassed the objective of 10 physicians per 10,000 inhabitants; the Spanish- and Portuguese-speaking region reports an estimated total of 753,984 physicians, 264,000 dentists and 355,106 nursing professionals and paramedics. Almost all countries report a slightly positive annual variation in the number of physicians, dentists, nursing professionals and paramedics: 8% in the Andean area (3% in Venezuela while Colombia reports twice that number); an average of 4% in MERCOSUR, with 5.4% in Brazil and 2% in Argentina; while non-Latin countries of the Caribbean continue showing the influence of a brain drain. Health workers in the region are mostly females and the trend continues to grow; in most countries women physicians are approximately one-third of the total.
Expansion and Development
The initial stage will be mainly oriented to the use of Internet, since the TV-signals in Internet will take more time in view of its obvious complexity. The requirement of excellence in the content of the project's educational material imposes the need of an organization with easy access to academic and professional centers throughout the region at appropriate levels of representation for a fair appraisal of the Project's value. Consequently, FEPAFEM will form part of the Project's Academic Board. Further, the organization that will manage the project must bear in mind the hardware and software obsolescence factor, in terms of new technology breakthroughs. There is a need of establishing from the start a close relationship with private suppliers of specialized services (outsourcing) because hiring services result less expensive than developing internal production capacity.
This field includes the provision of technical services for teacher training, editing and transformation to the virtual media of courses developed. The projected need of managerial, technical and administration staff has been kept at the lowest level required for ensuing the project and will be mostly provided by FEPAFEM and similar Institutions in keeping with a clear criteria of self-sustainability. The Project will have a supervisory and strategic direction body that will be called Strategic Academic Nucleus and is related to FEPAFEM, which is an organization that meets all the requirements and is represented in every country by way of the National Associations of Schools of Medicine of the region.
A Steering Committee, in charge of monitoring the educational quality of course contents, will also be entrusted with the receipt of initiatives concerning new courses proposed by local associations, the channeling of technical support offered for the development and adaptation of courses and a periodic evaluation of the project's progress. Its different functions will be:
1) Establishing a close relationship with health institutions,
2) Negotiating agreements with agencies that will support the courses,
3) Carrying out the initial marketing among the different state health systems, professional bodies and medical organizations that might be interested in supplementary courses,
4) Administering the Project funds and inform the contributing public or private agencies of progress achieved and goals met in accordance with the project's schedule,
5) Making the required contacts for entering into a contract with the Internet broadband carrier either for the provision of services or for the possible establishment of an association to develop the project in other countries of Latin America and the Caribbean.
The project will be initially developed as a pilot with the Schools of Medicine in Venezuela for a later expansion to other countries in Latin America and the Caribbean subject, in each case, to the availability of high speed Internet access capable of supporting the IP television protocol. Each country will require a feasibility study and a system need analysis as well as identifying the social organization capable and willing to be responsible for the project implementation. Financial viability of the Vi@Salud Project, that is, its continuity in time is subject to internationalization of the project; an activity limited to a country as small as ours does not warrant the investment. Therefore, success will be represented by a change from 50,000 to 80,000 potential users in Venezuela to 800,000 to 1,200,000 health professionals in the region.
Conclusions Geared to National and International Impact
In spite of several isolated attempts, an activity like the one projected does not exist in the Latin American region. The project that we propose: A technological platform of continuous education for health professionals coupled to an information system aimed at giving support to high level interactive education, is at present vital for optimizing the processes and reforms in the health sector. It is reasonable to expect the appearance or optimization in the near future of other alternatives, but it is not likely that these competitors will address the professional sector in the manner presented here, rather they will try to focus on consumers in general (patients) following the common practice in North America and Europe. A corollary of the above, which we give only as a reference, is that we face a small time window in a market with a high potential of growth and development and significant possibilities of economic return and sustainability.
The opportunities for developing in Latin America via Internet an activity useful to the health sector while remaining commercial and profitable are similar to those present in North America and Europe a few years ago. Although Web navigation and informatics applications are gradually consolidating in the region, telephone connection costs (principal means of access to the web) are still too high. Nevertheless, all indicators show a high and sustained growth of all activities related to Internet, in fact demographics of the market segment are largely favorable with ample possibilities of subsequent e-commerce.
Internet subscribers are mostly professionals with living standards well above average; if the current growth rate for Internet use and services in the region remains at 25% (a conservative estimate) for the next five years, the region will have 25,000,000 users by and large from the big countries (Argentina, Brazil, Mexico and also Colombia, Peru and Venezuela). The total population of Latin America in the year 2000, according to ECLAC, was approximately 520,000,000 inhabitants. In that same year, the United States had a Spanish-speaking population of 37,000,000. Spanish-speaking population of the Americas can be divided in four main regions, based on their historic and economic background (countries with less than 3,000,000 inhabitants are not included):
a) Hispanic NAFTA: Total population 135,881,000 Includes Mexico (98,881,000) and Hispanics in the United States (37,000,000). Traditionally, the latter are not considered Latin American.
b) Central America and the Caribbean: Total population 53,000,000. Includes Costa Rica (4,100 ,000), Cuba (11,200,000), El Salvador (6,300,000), Guatemala (11,400,000), Honduras (6,485,000), Nicaragua (5,074,000) and Dominican Republic (8,500,000).
c) Andean Region: Total population 104,610,000 Includes Colombia (42,321,000), Ecuador (12,460,000), Peru (25,662,000), and Venezuela (24,170,000).
d) MERCOSUR: Total population 240,100,000 Includes Argentina (37,100,000), Bolivia (8,500,000), Brazil (170,700,000), Chile (15,250,000), Paraguay (5,500,000) and Uruguay (3,500,000).
The incorporation of the product resulting from the project in the existing telecommunications media should be highlighted. This project has been designed for direct integration into tele-informatics media, with maximum use of basic tools for interconnection to Internet, either through a dedicated link (broadband) or by telephone connection, in which case there are two alternatives: Direct connection to Internet or direct connection to a server through a single national access number.
An educational project for the health sector constitutes a preamble for a more demanding and necessary activity: TELEMEDICINE. The term telemedicine stands for the use of telecommunications techniques for remote medical diagnosis and care. Digital communications technology is the means used for providing medical services to places generally deficient in resources and at significant distances from the service providers. However, the term telemedicine includes the simple use of phone and fax as well as the utilization of sophisticated systems with computers, fiber optics, satellites and other high-tech hardware requiring different kinds of software. At present, telemedicine is used to assist in the process of clinical decision making, to send medical information like X-ray films, EKG-tracings or other data with the purpose of performing real time examination of patients geographically apart. It also includes the use of these technologies for teleconferences, educational activities, capture of epidemiological data and optimization of educational processes because communication of relevant information is an integral part of any educational process. On its part, epidemiological surveillance systems that feed statistics and patterns of local morbidity and mortality are, by way of interactivity, by-products of a project of this nature.
It is reasonable to expect that those professionals whose activity is evaluated with systems intensive in information flow will become in the future specific subjects for distance education programs. On the basis of actually knowing the needs of a professional (analyzing his behavior with information systems) education can be streamlined to fit those individual needs.
In Latin America and the Caribbean, these new systems of information and medical communication must become the fundamental basis for developing the educational platform required by the health sector and its reforms. Certainly the objective is to contribute to the application and development of social justice, serving the underserved, both in urban and most specially in remote geographical areas, which could be achieved with the use of wireless broadband in strategic and practical alliance with major projects such as the Global University System being assembled with the UNESCO, as one promising and effective possibility of developing a worthwhile contribution in Latin America.
References
BELLCORE, white paper on investment priorities for the information infrastructure in Latin America and the Caribbean. (1998). Report to the "Informatics 2000" Initiative at the Summit of the Americas, Santiago de Chile.
Castells, M. (2001). La galaxia Internet, reflexiones sobre Internet. Barcelona, Espa--a: Empresa y Sociedad; Areté / Plaza & Janés Editores..
Castro de Moura, Claudio (1998). Education in the information age. Washington D.C.: Inter-American Development Bank.
Education in the Americas: quality and equity in the globalization process (1998). Washington D.C.: Organization of American States.
Field, M.( 1996). Telemedicine: a guide to assessing Telecommunications in Health Care. Washington: National Academy of Sciences Press.
La Salud en las AmÈricas (1998). Washington, D.C.: Organizacion Pan Americana de la Salud. (Publicacion Cient'fica n: 569).
Mandil, S.( 1998). TeleHealth. What is it? Will it propel cross border trade in Health Services Internationally? A development perspective, UN Conference on Trade and Development.. Geneva:UN-WHO.
Mosley, W.H., Bobadilla, J.L., Jamison, D.T. (1993). The Health Transition: implications for health policy in development countries. Oxford: Oxford Medical Publications.
OPS-PAHO (1998). Sistemas de informacion y tecnologia de informacion en salud. Desafios y soluciones para America Latina y el Caribe.. Wash.: OPS.
Packer, A. L. y de Castro, E.. (1998). Biblioteca virtual en salud. Centro Latino-Americano y del Caribe de informacion en salud -BIREME-/OPS/OMS. Sao Paulo.
Potashnik, M. y Capper, J. (1998). Distance education: growth and diversity. Finance and Development. pp 42-45. March.
Pulido P. M. (1998). Universidad Virtual de Ciencias de la salud de América Latina y el Caribe o Proyecto Vi@Salud, Estudio de Factibilidad., FEPAFEM, Caracas, INTAL-BID.
Pulido P. (1997). Medical practice and medical education in Latin America. Education for Health. Vol 9. No 3 286-306. 1996. Pulido P. A. Salud Proyecto Nacional. Revista SIC No 600. 502-508.
Pulido P. (2003). Tiempos de cambios en educacion medica y servicios de Salud para responder a las necesidades de la poblacion Revista Internacional de Educacion Médica, Vol.6, p.6, Suplemento 1, Enero-Marzo.
Pulido P., et al. (2002). Telemedicine and medical / health education, Ch. 4 en Telemedicine Journal and e-Health. 8. (1), 49-60.
Requena J. y Pulido P. (2001). La Universidad Virtual en Ciencias de la salud de América Latina y el Caribe. fundamentos y viabilidad. medicina. Revista de la Academia Nacional de Medicina de Colombia. 22 No. 1 (32), 32-43. 2000 y revision en "Informatica, Educacion y Salud en la Sociedad del Conocimiento, FEPAFEM-COLCIENCIAS-ACADEMIA DE MEDICINA DE COLOMBIA, Bogota.
Requena, J. (2003). Tecnologia de la educacion a distancia para la salud. XVI Conferencia Panamericana de Educacion Médica, Buenos Aires, 2001 y Educacion Medica --International Journal, 6 , suppl. 1, 69-71, Jan-March.
World Bank,
o World development report: Investing in health (1993). New York: Oxford University Press.
o Fiszbein, A., Lowden, P. (1999). Working together for a change, Economic Development Institute.
o World development report: knowledge for development (1998-99). New York: Oxford University Press.
o Perspectives on development (2001-2002). Winter.
Author Biographical Sketch
|
Dr. Pablo A. Pulido M. Executive Director PAFAMS, Panamerican Federation of Associations of Medical Schools Former Minister of Health, Venezuela Apartado de Correos 60411 Caracas 1060-A VENEZUELA Phone: +58-212-945-0857 Fax: +58-212-945-4275 E-mail: pablopulido1@compuserve.com |
|

Pablo Pulido, M.D. is a Physician, Internal Medicine-Cardiology. Founder of Centro Medico Docente La Trinidad, a non-profit teaching medical Center in Caracas. Was Secretary of Health and Welfare in 1993-94 and later on 94-98 member of the National Health Council in Venezuela. Currently Executive Director of PAFAMS, Panamerican Association of Medical Schools with 389 affiliated Institutions in the Hemisphere. Founder of the Metropolitan University, a Technical Institution in Caracas with strong orientation in engineering, business administration and education. President of the Metropolitan University Foundation Board of Trustees. Additionally is Vice President of The Foundation of Popular (low cost) Housing and Member of the Board of Governors, Mendoza Foundation in Caracas.
Other activities include the Global Advisory Board of the Thomas Jefferson University, Philadelphia; former International Member of the Scientific Advisory Committee, Novartis Foundation, London; David Rockefeller Center for Latin American Studies, International Advisory Committee, Harvard University; Steering and Advisory Committees, Institute for International Medical Education, China Medical Board, NY; Fellow American College of Physicians; Ass. F. American College of Cardiology, Venezuelan Society of Cardiology; Board Member of International e-Health Association, IeHA.
|
Jaime Requena, Sc.D. Fundacion Universidad Metropolitana Program Advisor, PAFAMS Caracas, Venezuela Tel: + 58 (212) 242 3087 E-mail : jrequena@unimet.edu.ve |
|

Jaime Requena is 56 years old and was born in Venezuela. He is a Biologist and obtained a Ph.D. degree in Physics and Chemistry from Cambridge University (England). He has held administrative positions of high responsibility in his country, having been the Director of the Instituto Internacional de Estudios Avanzados (IDEA) and its International Center for Scientific Cooperation, and UNESCO Regional Center. He has received several distinctions, among them a Special Mention of the Organization of American States "Manuel Noriega Morales" International Prize for Young Researcher in Biology. In 1994 he was elected "Simon Bolivar" Professor at the Chair of Latin American Studies of Cambridge University and Professorial Fellow in Churchill College. In 1997, Cambridge University awarded him a Sc.D. degree in Biology. He is a Member (Chair XXVI) of the National Academy of Natural Sciences, Physics and Mathematics of Venezuela and of the Third World Academy of Sciences of Trieste, Italy. He is the author of over 60 papers and numerous Review articles, which have appeared in reputed international Journals. His research has greatly contributed to the quality of science in his country and in Latin America.