In Global Peace Through The Global University System
2003 Ed. by T. Varis, T. Utsumi, and W. R. Klemm
University of Tampere, Hameenlinna, Finland
VIRTUAL REALITY ENVIRONMENTS FOR EXPERIENTIAL LEARNING IN THE SCIENCE AND MEDICAL DOMAINS
University of Twente
Abstract
The spectrum of instructional strategies has widened in scope into the vast still unexplored area of mixed-initiatives between expert-like performance models and the more autonomous student who carries his/her own agenda and learning styles. Virtual Reality (VR) is becoming a serious candidate for a learning environment for complex skills like vascular interventions. The diagnostics, dimensioning and insertion of the endograft stent has been modeled as a decision making process and now faces its implementation in a VR learning space. Beyond the topological and morphological aspects, it is the orientation and navigation in earlier-performed successful interventions that offer the opportunity for a competence-based learning process before the candidate surgeon enters the clinical stage.
Introduction
Since Constructionism and constructivism have entered the arena of learning paradigms, the discussion on its impact has been mainly ideological and not so much empirical or pragmatic. As many educational and training projects tend to build upon the trend to give more autonomy to students, it seems necessary to make more precise architectures and in-depth interaction recipes for defining the balance between the two extremes: System control versus student control. This chapter presents both the formal and pragmatic rationales behind new virtual environments for learning. The DIME project (Distributed Interactive Medical Exploratorium for 3D Medical Images) aims at conceptualizing, implementing and researching the effectiveness of a VR-based pre-surgical planning and teaching environment. The DIME explorations aim at a pre-surgical planning and teaching applications, which will most likely result in better post-surgical results, lower health care costs and increased efficiency in the training of fellow-surgeons. The project is a collaboration of a 'computer science' group from the University of Amsterdam (UvA)[1], a 'medically oriented computer science' group from the Leiden University Medical Center (LUMC)[2], a 'cognition' group from the University of Twente (UT) and medical specialists from LUMC) and The Medical Spectrum Twente. A VR-based pre-surgical planning and teaching environment is proposed for novice surgeons. Although this environment is generic and can be put into practice in any medical specialisation where such 3D imaging techniques are in use, in this project we specifically focus on vascular surgery. This environment will be developed as part of the DIME project (Distributed Interactive Medical Exploratory).
Surgical Training in Virtual Reality
The surplus of surgical training skills as well as being oriented in medical disciplines like anatomy, histology, physiology, etc., is evident. The optimization of its professional training elements needs to most complete repertoire of learning technology like the media spectrum and the full repertoire of new learning paradigms. The aim of this paper is to show the compatibility between the most advanced visualization methods currently feasible for the average desktop work stations. The overall conception is that the clinical training will gradually be extended with VR learning systems, in order to make the supervised real operations more effective and safe.
Relevance of Virtual Reality
- Surgical techniques have become increasingly complex, thus making the learning curve to master these techniques steeper and longer.
- More complex intervention techniques are rapidly developed and introduced in the daily practice.
- The conventional surgical teaching method is a close daily working relation between the experienced teacher (trainer) and the unskilled pupil (trainee).
- In traditional teaching the steep learning curve takes place during the interaction with real patients.
- The modern patient does not accept any mutilation attributed neither to the disease nor to the intervention.
- It is clear that a perfect preoperative visualization and planning, and rehearsals of these interventions are essential.
- This means that while there is an increased demand for surgical training, experienced surgeons have increasingly less time and opportunity to cope with this demand. A dedicated medical VE is badly needed to lift this burden from their shoulders.
- Of importance is also the possibility to allow trainees to explore critical situations and to let them experiment with an underlying model of the phenomena and processes in the human body, without the stress of having to deal with an actual patient.
- Virtual surgical tools should be available for life-long medical education and assessment of the surgical consultant.
- Based upon the disappointing experiences with "Intelligent Tutoring Systems" in the 1980s, we do not want to undertake the paradigm of "training dummy mannequins" as it lacks the notions of "continuous learning" and the "surgeon as active problem solver".
The Urgency for Laparoscopic Interventions
More complex intervention techniques are rapidly developed and introduced in the daily practice.
Nowadays the laparoscopic cholecystectomy is the preferred technique in many hospitals. However, the majority of the surgeons performing laparoscopic cholecystectomies are autodidactic. They heard about the technique on congresses. They visited clinical demonstrations in centres of excellence. Thereafter they planned the first procedures in their own hospital. It is not surprising that the results are not as good as reported in the literature in the early periods. The steep learning curve is derived from patients. A sufficient training and formal assessment of the surgical team before introducing the new technique into the hospital is not available. Moreover, more complex intervention techniques are rapidly developed and introduced in the daily practice. An example of this is the endovascular exclusion of infernal aortic aneurysms with an endograft. Cuijper recently reported in his thesis that only after an endovascular experience of 30 electively treated triple A the complication ratio is sloping down to acceptable levels. In the Netherlands only a few hospitals have such an experience. Also the first ruptured aortic aneurysms are treated in the endovascular way with a very good outcome. However, this emergency procedure demands a large endovascular experienced team available during day and night. Gaining enough experience with this procedure is not possible in most of the hospitals in the Netherlands. Unfortunately, it is not possible to transport a patient with a ruptured triple A to centres of excellence because of hemodynamical instability. In other words, the patients do not survive delay of treatment due to transportation. The next generation, more complex endografts with the possibility of perirenal sealing is underway. The results of the first clinical experiments came from "down under". It is clear that a perfect preoperative visualisation and planning and a dummy operation of the whole procedure is essential.
The Urgency for Training in Virtual Reality
The conventional and still actual surgical teaching method, introduced more than a century ago, is a close daily working relation between the practised teacher (a consultant surgeon) and the unskilled pupil (the surgical resident). Working-weeks of 70 to 90 hours were accepted and after 6 years of gaining theoretical and especially practical skills under direct supervision of the consultant the resident becomes a surgeon. Nowadays our society does not accept such long periods of formal learning and the working week is shortened to a maximum of 48 hours. This results in a 40% decline of directly supervised practical experience of residents in their first years of surgical training. Moreover, the government asked the surgical society to offer the basic surgical training in only 5 years! On the other side, the same government makes laws as the BIG and the WGBO. The surgeons are obliged to be qualified (formal licensed) and to be skilled and properly trained to offer and execute an intervention to or on a patient. Due to the "Schengen convention" there is a right of free establishing of the citizens of the European community in the participating countries. The formal training of resident and consultants in the European countries showed large diversities. Objective and proper methods for assessment and comparison of the outcome of the surgical training in the European countries are not available. It is clear that the conventional surgical teaching methods do not fulfil the demands of patients, the society, the government and the surgical profession. New training methods have to be developed. The development of virtual reality surgical tools for theoretical and practical training and assessment of the resident is urgent. Moreover, virtual surgical tools should be available for life-long medical education and assessment of the surgical consultant maintaining a high level of expertise and skills in the profession. This project intends to contribute to the steep increasing need for practical training and objective assessment for the surgeon in training.
Goals of the DIME Project
- To create a VR learning environment that allows surgical trainees to practice their skills in the Operating Room Virtual Environment (VE) and to enhance their understanding of the procedure under study by using the Library VE or the peer-to-peer chat function.
- To identify the more objective training elements that need to be conveyed before the constructionistic learning starts. This is the reason that the first stage arranges teams with the various expertises that play a role for the definition of the anchoring points in the training of the future surgeon.
- To define a generic instructional method that intermediates between a VR medical model and a novice who needs to understand and optimize its functioning.
- To specify and evaluate VR elements for the pre-clinical training phase of novices in artery surgery.
An Expert System for Risk-evaluation
of Endovascular Stent Prosthesis Placement
The VREST[3] group has undertaken the formalization of dimensioning the stent orthesis for the AAA patients. In order to obtain an uncomplicated passage and a lasting exclusion of an infrarenal abdominal aorta aneurysm (AAA) through endovascular placement of a stent-prosthesis, one has to take into account many unique anatomical properties of the aortic-iliac-femoral trajectory and many unique properties of the stent prosthesis.
The chances for successful sealing were independently expressed in "complication rating" for each AAA by five clinicians and the expert program. The complication rating was divided in 0% to 59% (low to intermediate risk), 60% to 94% (intermediate to high risk), 95% to 98% (very high risk), 99% (practically impossible) and 100% (impossible) to obtain sealing. It was allowed to choose between all configurations of three commercially available stent-prostheses. A total of 3030 AAA assessments were given by the five clinicians. These were compared to the assessments of the expert system.

Figure 1. Abdominal aorta aneurysm anatomical data input screen
Table 1. Correspondence between the assessments of the clinicians and the expert system
|
|
Agreement |
False positive |
False negative |
Discussion |
|
Surgeon 1 |
73.4 |
0.0 |
1.7 |
24.9 |
|
Surgeon 2 |
75.5 |
0.7 |
2.5 |
21.3 |
|
Surgeon 3 |
73.7 |
0.0 |
1.8 |
24.7 |
|
Radiologic 1 |
70.6 |
0.5 |
4.2 |
24.8 |
|
Radiologic 2 |
64.8 |
0.0 |
8.1 |
27.1 |
|
Total |
71.6 |
0.2 |
3.7 |
24.6 |
Agreement: Same advice clinician and expert system.
False positive: Advice clinician = no intervention, advice expert system = intervention.
False negative: Advice clinician = intervention, advice expert system = no intervention.
Discussion: Advice clinician = high risk intervention, expert system = no intervention
Results and Preliminary Conclusion
There appeared to be a good correspondence between the assessments of the clinicians and the expert system as finally visualized as in Figure 2. Specifically the chances for an incorrect positive advice from the expert system are minimal (1:500 assessments). In case of a high complication rating the expert system tends to advise negative on stent placement in more cases than the experienced clinician does.
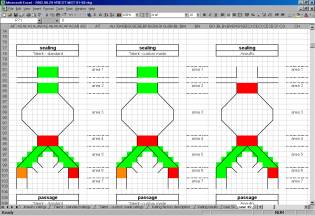
Figure 2. Discrete modeling rational for the go-no go and the
dimensioning of the stent artifact
The basic underlying rational for the go-no go and the dimensioning of the stent artifact has been certified in this way. The envisaged DIME project plans the support of the 3D aspects of the particular patient in concern. Both the experienced and the novice vascular surgeon will increase effectiveness and task efficiency as the MRA images are transformed into three-dimensional models that can be inspected for critical morphologies and to anticipate better to the actual medical intervention.
VR for Learning
The Need for Visual Orientation
As computer-based visualizations like those in VR and modelling for design and idea generation becomes more common, the research interest may shift forward into a new and highly intriguing field. It is the question how to promote a new type of visualization that is based upon human conceptual imagination rather than the conventional perception of the 3D world around us. It is not an essentially new step, because we extended our naturalistic way of displaying what we saw into the more or less abstracted indication of what we take as crucial behind the meaning and impact of the issue: quantitative graphs, schematic displays of complex functioning and not to forget the topographical map itself. Maps may suggest that you see a landscape from a bird's perspective. However, we soon perceive that without filtering and articulation there is no conveyance of thought and navigation. As visualization techniques develop, we attempt to display conceptual entities rather than reminiscences to objects and physical space. Concept mapping is the more salient exemplar in this new line (Kommers, 2003). The paradigm is that any mental entity or process may appear in a spatial configuration of both concrete and abstract ideas. The further formalisms how to control expressiveness and topology by pruning and zooming is a matter of conventions that should fit in the contract between a task, its user and the concrete representational device like a white board or a computer screen. Some tasks inherently aim at configurational awareness like planning, decisions making etc. Some tasks address the more intuitional stages of human thinking like learning, persuasion or worshipping. Concerning learning and teaching, the so-called instructional approach has almost become synonymous with effective cognitive growth. In the more recent years we see however that the cybernetic aspiration of the 60-70s has mainly led to an over-organization of study programs and students complaining that the school is like a factory and at the same time like a hospital. The term "existential learning" attempts to indicate its complement: The student is the main character his longer-term development. We again start to accept that learning has a lot to do with mental and emotional growth in which information access plays only a subordinate role.
Learning in a Virtual Spatial Reality
The tendency to allow trainees to explore critical situations and, in case of medical students, to let them experiment with an underlying model of the phenomena and processes in the human body, is not new; (Psotka, 1995, McLellan, 1993). There is a considerable amount of evidence that training by computerized models facilitates the learning process (Moshell and Hughes, 1994). Also we see a growing interest for offering fully 3D environments that allow a continuous fading between the full realistic reality like looking through glasses to the real patient and at the other side seeing the superimposed vectorized model of the same patient but now with only the structure of the blood vessels (and if available, the computed blood flow and the animated pressure on critical spots). In the pre-service training novice surgeons may primarily explore the models at the vector side of the spectrum. As more experience builds up the captured videos of the same patient may become involved. Finally students may undertake real operations, supervised by a specialist. As this stage of the training is costly, it is quite desirable that an intense VR stage of the learning has taken place. In this project we will establish the most effective instructional sequence in the VR-based training simulation.
Learning Paradigms Benefiting from VR
The traditional approach to optimise learning through "just-in-time" information and feedback can be summarised as instruction. As the trainee has a larger repertoire of prior knowledge and skills, this "cybernetic" approach has the disadvantage of not enough stimulating the meta-cognition and the potential to learn-to-learn by the trainee; (Kommers & Zhiming, 1998; Kommers, 2000). The complement and to a certain extend the alternative for instruction is learning by construction. Constructionism is the awareness that learners undergo a highly personal process, due to their cognitive style, various ways of mental imagination and differences in prior knowledge as well. Under this paradigm, trainees in surgery need the opportunity to acquire a model like the rules underlying the trade-off in artery intervention, in an unthreatening situation with a larger bandwidth for experimentation and reflection, before the actual practice with real patients take place. The connotation of constructivism is that the learner actually builds his/her conceptual knowledge upon prior analogue knowledge. In case of artery surgery, models from hydrodynamics, the principles in flow theory and many more, play a crucial role. Besides that there is a set of specific facts that play a role around blood vessels. During learning, the trainee attempts to reconcile earlier experiences with factual rules as formulated by experts in the field.
- If the factual data dominate the trainees' intuition and imagination, we may expect that his/her performance later will be brittle and not flexible enough for the large variety of complex situations.
- If the trainee relies too heavily on similar domain knowledge and intuition, there may arise a discrepancy with the "golden rules" and the statistical lines based upon experience among the colleagues. Also the more or less standard operations may not become automated and the communication with colleagues about taken decisions may become troubled.
In the underlying project proposal, the first stage of Medical Consultation aims at identifying the more objective training elements that need to be conveyed before the constructionistic learning starts. This is the reason that the first stage arranges teams with the various expertises that plays a role for the definition of the anchoring points in the learning of the future surgeon.
From an Informational to a Conceptual Approach
Before further highlighting the need for conceptual rather than instructional representations it is useful to stress that already in pre-instructional learning theories the notion of meta-cognition has played a dominant role. Ann Brown (1994) has systematically brought forward the dominance of cognitive development, intentional learning, transfer of learning, meta-cognition and self-regulation.
"… Learners came to be viewed as active constructors, rather than passive recipients of knowledge. Learners were imbued with powers of introspection, once verboten. One of the most interesting things about human learning is that we have knowledge and feeling about it, sometimes even control of it, meta-cognition if you will.………
…….. Those interested in older learners began to study the acquisition of disciplined bodies of knowledge characteristic of academic subject areas (e.g., mathematics, science, computer programming, social studies, and history). Higher order thinking returned as a subject of inquiry. Mind was rehabilitated…."
The "cognitive apprenticeship model" (Collins, Brown & Newman, 1989) is another illustration of the shift from guidance to self-control; it claims that effective teachers involve students in learning by problem confrontation even before fully understanding them. Essentially you may say that learning is in fact the recreation of earlier cultural processes and evidences. Though this is an expensive phenomenon, it has the power of revalidation, as learners will also check the presented expertise against their own experiences. Also the regeneration facilitates the knowledge activeness during life; simply storing and remembering transmitted ideas is less adequate to pop-up in new problem settings. The intriguing question is how we rely on pictorial, schematic and iconic images during this process of intellectual "reverse engineering." Is there any pre-arranged repertoire of visual grammar or should we stimulate learners to re-invent one's personal semiotics for conveying the learning process.
Concept Mapping for Navigation in a VR Learning Environment
The fast growing attention for multi-modality, full 3-dimensional VR (Virtual Reality) and the avoidance of anisotropy has partly supplanted the designer's attention for the students' conceptual states. One additional promising aspect is to prepare and structure the VR course for Educationalists on the Web and bring an overview of ongoing research into the urgent question how to orient students in conceptually complex domains using VR. The central theme to give an overview of VR learning environments that enable learners to explore new physical spaces, but even more important: To let them experiment with new materials, complex processes like kinesthetic, extruding, casting etc. VR becomes a substantial and ubiquitous technology and subsequently penetrates applications for education, learning and training. In addition to multimedia, VR places the user in a 3 dimensional environment. The user feels "in the middle of another environment." Most of the VR systems allow the user to travel and navigate. More promising for learning purposes is to let the user manipulate objects and experience the consequences. This paper introduces the potential impact of 'immersion' for learning environments, the current state of the art in VR, its drawbacks, the overall metaphor of virtuality and the most feasible application areas. The main section of the reporting is the research agenda for VR in the next coming years. The recommendations involve VR and collaborative aspects (MOOs), its integration with video conferencing, drama and constructionism, temporal awareness, and finally the integration into special curricular topics. The targeted goal of this paper is the gradual embedding of VR elements in current research and developmental practices. Especially fast propagation of WWW-based tele-learning can benefit from the VR prospects in the coming years, as VR programs can now be accessed by the most common web browsers like Netscape and Explorer.
Throughout the many stages of media they have helped us to extend our perception, imagination and manipulation. VR is just an extra step on the long road bringing the imagination as close and realistic as reality itself. After the first experiments in the fifties with complex kinesthetic devices like multiple cameras, senso-motoric devices and even smell generators, more elegant head-mounted devices were developed in the early nineties. Both defense research and the computer games industry were the main stimulators of VR so far. It is hard to describe what VR is not: It encapsulates all previous media, even books, slides, pictures, audio, video and multimedia. The typical contribution of VR is its effect of immersion; The user feels as if (s)he is in a different world. Both the sensations and the actions of the user should resemble as much as possible to humans in a normal physical environment; Seeing, hearing, feeling, smelling, tasting; but also speaking, walking, jumping, swimming, gestures and facial expressions. The VR utopia means that the user does not perceive that a computer detects his behavior, and also that he perceives the real world. The generation of proprio-ceptive and kinetic stimuli is only possible if the user is placed in a tilted room like the hydraulic controlled cabins for flight simulators. The generation of taste and smell, and the realistic enervation of the human skin as if one touches an object or another person may be one of the most challenging and complex steps for VR to take in the next years. Augmented reality occurs when the user faces the real world, but on top of that the VR environment superimposes a computer-generated message in order to assist the user to perform the right operations.
VR is a desired technology for those applications in which reality that does not exist (yet), cannot be accessed, or is too dangerous or expensive to betray. As for many of the today's VR proponents, "Reality" sounds as the only inevitable physical world; they rather prefer 'Virtual Environments'. This term articulates the view that based upon one's responsibility and perspective we postulate different (real) worlds. Because of the term Virtual Reality, however, we will maintain the term VR. Computers are inherently tools to emulate real situations and environments. VR in its current shape suggests to users that they are in a fictitious environment. The next generation of VR will suggest that you can really walk around there, and can manipulate and experiment. This environment does not necessarily need the same properties as the real world. There can be different forces, gravity, magnetic fields etc. Also; in contrast to the real solid objects, in VR the objects can be penetrated. The properties of a good VR are like those of a good teacher; it allows the student to explore the basic laws of a new domain; Location, scale, density, interactivity, response, time and level of intensity can be varied. It is not necessary to explain what the VR user sees, hears, feels and finally smells. Also textual descriptions are not optimal for this learning by intervention, as text (and also hypertext) is essentially not apt to describe complex spatial phenomena. In this sense, VR gives a substantial contribution to interactive learning environments; it combines the realism (like in a video recording) with the manipulative (fictitious) reality like in simulation programs. We may expect that within 10 years, VR will be the default presentation mode of computer applications in general. Besides the visual/auditory and spatial aspects, VR can also provide support in the navigation through concept space. In this case, the dimensions are no longer limited by the Euclidean geometry: they can represent mental perspectives, rules and dependencies. Virtual space allows traveling through a 3-dimensional concept map. VR is a three-dimensional simulation technique, which becomes more important as:
- Mistakes during the learning process becomes more dramatic,
- Reality itself cannot be accessed,
- Parts of an emulated reality have to be smudged.
There are at least four VR aspects of importance for the perception by the learner:
1. The mechanism of avatars. They represent the user in a fictitious environment. Even the expert teacher should be represented in one-way or another. In the scope of the DIME project the avatar is integrated by making the demonstration of the many expert interventions available so that the learner can smoothly orient to the master solutions and gradually absorb the specific rules and conditions for the exceptional cases
2. The mechanism of affordance. This is the user's ability to orient in a new world, based upon distinguished features. According to Norman (who refers back to J..J. Gibson (See Beck & Cunningham, 1989), affordance is a relation between an object in the world, and the intentions, perceptions and capacities of a person. As an example he mentions that a door with a push button instead of a handle for pulling, has the affordance to push the door.
3. Man-machine Interface. This interface gets an ever more prominent position. Initially the user interface was a kind of serving hatch between the user and the system. In case of very interactive systems sometimes one speaks about user intraface; in this case the whole application establishes the manipulation space for the user. The user's intuition then needs to be sufficient to instruct the user. The user should not need meta-communication in order to understand the program's potential.
4. Immersion. The confrontation between the learner and the new (physical) environment should be 'immersive'; Rather than seeing a flat display, the user should feel himself in the VR. Especially if the task concerns complex three-dimensional orientations like surgery and rescue expeditions in complex areas, then a VR exercise is quite useful before going into reality itself.
Concerning the relevance of VR for education and training, two aspects have to be taken into account:
1. VR is a default component of the user interface in the future. The desktop metaphor was a revolutionary one, as it took the human's physical (spatial) reality for the organization of information in general. As long as it concerns 2D documents, this is a lucky choice. As soon as the user behaves in a 3D world, a more dynamic representation is needed. Also the acoustic consequences of moving through space should fit; the sounds' amplitude, reverberation- and Doppler effects as one recedes or comes closer to the sound source, should resemble the reality.
2. The second is that the ability to increase realism also implies the possibility to introduce a specific element of non-realism. One can confront the student with an alien world and make it stepwise more or less realistic. Basic nature laws can be explored, like mechanics, chemistry, electromagnetic fields, etc. Viewed from a constructionist perspective, VR has an important function in the realization of understanding complex processes; The student is allowed to orient in several directions and subsequently find a way through the information space.
Educational VR systems seem to be a natural extension of computer-based simulations nowadays. The basic approach is to allow students to explore and discover the fundamental laws in a new environment and domain. For the initial confrontation with new tasks and for the stage of exercising, this approach seems logical and consequent. The effectiveness of the training for the mastery of the final task in reality is a subject for further research. Based on similar developments in interactive video, multimedia and telematics, it is not desirable to wait-and-see until the technology development has 'finished'. Educational and training research should keep pace with the newest VR systems and think along its new potential for learning. Can VR be an Effective Tool for Education or Training? The answer depends partly on one's definition of VR and partly on one's goal for the educational experience. It may not be worth the cost if the goal of the educational experience is simply to memorize facts. However, if the goal of the educational experience is to foster excitement about a subject, or to encourage learning through exploration, or to give students a taste of what it is like to be a research scientist, then VR may be worth the expense. It seems an interesting option to take the VR technology as a candidate metaphor for learning environments in general. That's why we introduce the more generic idea of "Virtual Learning Environments' in later stage of this article. Today it is a developing technology seen primarily in research labs, theme parks, and trade shows. Tomorrow it may be as common as television. Lanier (1989) likes to say that VR is a medium whose only limiting factor is the imagination of the user.
Learning by Exploration
Building upon previous and current research, the DIME project aims at the further evolution into a training support system that orients novice surgeons to explore and learn the critical dimensions in the anticipation of blood vessel transplantation and the placement of a stent or a by-pass. The project covers the data delivery, medical, VR-interactive and instructional procedures. The transformation into a training support system needs two stages.
1. Medical consultation: The collaborative use of VA by medical experts who discuss and negotiate about the interpretation of 3D visualisations of a patient's artery system. The calculation of the pulsatile blood flow and the deduction into shear stresses on the vessel wall is an important but not satisfactory argument to decide upon medical intervention. This stage of the research aims at a multidisciplinary collaboration between actors from the various medical disciplines, VR specialists, imagery experts and the training designers.
2. Instructional design: The design and implementation of a learning system that allows novices to prepare themselves for the supervised in vivo operations. The system should both allow a tutorial situation, where the experienced surgeon explains and demonstrates the key functionality and simulation mechanism. But also the trainee should be allowed to make an in-depth tour through specimens of the cases. After this phase, a wrapping-up conversation with the expert and the trainee should be completed, eventually leading to the stage of supervised interventions in real patients.
A large part of the test bed is dedicated to the learning / teaching goal, as it is an articulation of the much wider potential such a system has for research in general. A relevant side effect of VR-supplied training situations is the fact that it allows a smooth transition between being locally present in the training VR versus participating via telematic facilities at remote sites. Looking back to the logged students' actions may enable the trainer to decide upon the trainee's qualifications before entering a real operating room.
Initial Architecture of the Proposed VR Learning Context
The surgical skills and their continuous sophistication; how should it benefit ideally from the virtual Operating Room? In this practice "space" (at the right side of Figure 2) the cycle goes around diagnosis, prepare and execute the intervention. But at unforeseen moments we expect that students consult a library of domain expertise. Based on the log data generated by this VE,
- the coach and trainee can evaluate his/her progress and set out an appropriate personal learning path;
- the coach can extract general trends in learning of his/her trainees, as well as differences in learning styles of individual trainees.
Though this architecture looks adequate and robust, we decided not to adopt it basically, because of the suggested antagonism between the two. More adequate and fair seemed the model where the central core of the learning between the various approaches was due to variations in patients and the subsequent surgeon experts and the various trainees.

Figure 3. The interplay between the students' theory versus skill-driven learning
The alternative to the theory/practice model above was left behind and the key idea for the VR training space was called "Interconnected Expertise". It aims to create for the novice a quasi continuum of surgical interventions. Learning in this space allows a fluent transition between patients, surgeons and various stages in the intervention. It seems natural to trace the treatment by one surgeon in one patient through the natural chronology of the operation. But there are good reasons to switch between patients, as it shows typical morphologies that clarify the reason why the initial treatment was needed there.
Imagining VR As Interconnected Expertise
VR as representation of the targeted object world may be propagated sufficiently. More intriguing is the question how learners may benefit from the prior experts and successful peer-learners. This question was recently addressed and came to the idea that three main dimensions need to be articulated before a meaningful navigation by the learner may take place.

Figure 4. Three main dimensions for allowing the learner to navigate in prior vascular interventions
1. The first dimension (called Cases) is the set of indexed patients who vary from reflecting the prototypical standard medical problem as listed in the study books; in this case the abdominal aorta aneurism is clearly there, but with a minimum of complicated side effects and the patients is in a good overall condition. At the other end of the continuum there is the patient who suffers from a severe AAA phenomena, but at the same time a large number of constraining factors can be discerned like stenosis, aneurisms before and after the bifurcation and a complex artery morphology in the range between the stent insertion point and the place of stent placement.
2. The second dimension (called Trainees) varies between the highly-experienced vascular surgeon who performed in the Endograft stent VR model quite punctual and highly correct AAA interventions, to most of the embedded cases. At the other end of this dimension one can find recorded AAA interventions by freshmen demonstrating the many thinkable flaws. At each of the suboptimal interventions the ultimate surgeon marked the reason of labeling the flaw as being suboptimal and activates links to the real good solutions that should have been made.
3. The third dimension (called Episode 1..n) captures the subsequent stages in the AAA intervention. Two criteria for ordering them can be taken: The chronology of sub actions from early to later, versus the ordering from easy to complex. Analytical and experimental validation still needs to be performed in order to make a sensible choice here. In any case following the strict order of this dimension allows the learner to follow the prior interventions in it chronological order.
TwoCents: A self-learning VE for surgical training
Based on the arguments following in the rest of this chapter, a Virtual Environment is proposed for surgical training. New is the use of a dynamic database that gathers annotated experience of previous users in such a way as to open a direct, adaptive and relevant frame of reference for the trainee. This framework could be of use in other VEs as well, especially those which prepare trainees for work in environments where knowledge of different complex procedures and the ability to correctly assess a complex situation is critical.
Relevance of medical simulations
The field of surgical knowledge is becoming increasingly complex, due to several factors:
- More pathologies are candidates for surgical treatment.
- More specific techniques for different cases are being developed.
- The techniques themselves are becoming more complex, due to:
- the continuous creation of more sophisticated equipment.
- the patient's expectation of the outcome of the procedure (loss of function is hardly acceptable).
- The increasing age of patients ready for surgery adds further complexity to surgical procedures.
- Because of the factors mentions above, the 'turnover' of surgical techniques is getting higher.
As a result, the learning curve to master these techniques is getting steeper and longer, and in addition a need for life-long learning emerges. Two educational practices are recognized in conventional surgical learning.
One is the conventional surgical teaching method: a close daily working relation is established between the experienced teacher (trainer) and the relatively unskilled pupil (trainee). In a setting where more trainees must learn more in less time, this places an unrealistically high burden on the trainer. This is also rather costly. The other is related to the way new techniques find their way to the clinic: surgeons hear of new techniques at congresses, through demonstrations in centers of excellence or through the literature, and decide to implement these techniques in their own practices. This often leads to a period of trial-and-error before the new technique is well established, which obviously is not beneficial for the patients. The lack of sufficient training opportunities and formal skills assessment in this scenario is problematic.
The disadvantages of both training methods could be overcome using a Virtual Environment for surgical learning and skills assessment, and, as could be expected, considerable work has been done in this area.
TwoCents: Outlining the project
The heart of TwoCents will be a dynamic, annotated database that can be investigated by the trainee. This database is imagined as a cube; a three-dimensional form reflecting the next dimensions:
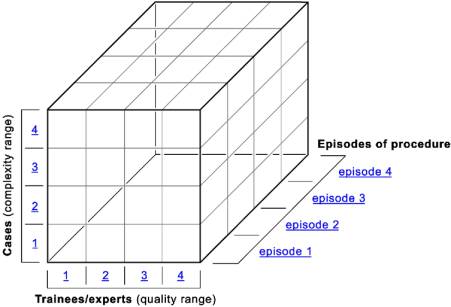
Figure 5. The dynamic, annotated cubic space for learners' navigation
- the X-axis represents generalized surgeons with differing levels of expertise (made anonymous)
- the Y-axis represents different medical cases, each different in complexity and optimal surgical strategy
- the Z-axis represents the different episodes or actions that constitute a procedure
An episode always consists of a scene taken from the procedure of a specific case with a specific trainee, what this trainee has done in that scene, and the annotations of the VR-root and other VR-users to that scene. These annotations can consist of written notes, video material, animations, photographs and graphics.
- Since navigating the cube is almost identical to interrogating it's content, in the following exposé navigational strategies are used as guidelines to the cube's functionality.
- Point-click once & press-enter on any cubette brings the corresponding episode on-screen.
- Point-click once on one cubette and shift-click once on another cubette selects both cubettes. When up to four cubettes are selected, press-enter opens all episodes in a split-view.
- When more then four cubettes are selected, press-enter brings annotated thumbnails on screen (each thumbnail corresponding to the selected episode). These thumbnails can be selected and activated in the usual way to bring the corresponding episodes on screen.
Double-clicking a cubette selects the cubettes that lie in a row behind that cubette, in a plane orthogonal to the side from which the clicked cubette was advanced. Press-enter brings this row on screen as a field of annotated thumbs.
Clicking any link (in the figures: {1, 2, 3, 4} horizontal, {1, 2, 3, 4} vertical or episode{1, 2, 3, 4}) brings the corresponding plane on screen as a field of annotated thumbs (See Figure 6).
So, depending on the plane from which the cube is advanced,
- A complete procedure from one trainee for a specific case can be assessed (Fig. 7).
- All trainees for one case and episode can be selected, allowing assessment of the surgical strategies of different trainees for an episode in a specific case (Fig. 8) or
- All cases for one trainee and one episode can be selected, allowing assessment of the surgical strategies of one trainee in the same episode on different cases (Fig. 9).
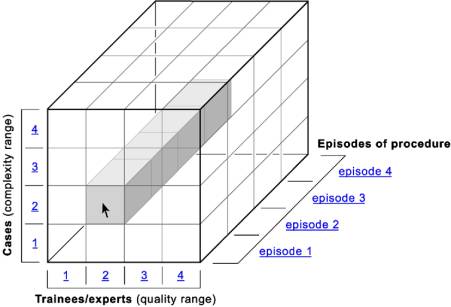
Figure 6. Selecting a Trainee / Patient intervention history
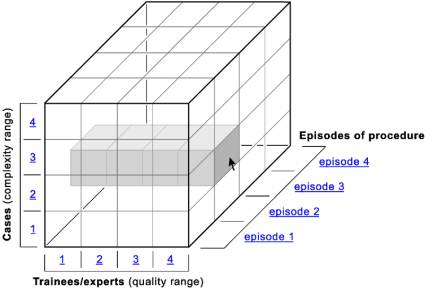
Figure 7. Selecting a particular intervention episode across all trainees for one particular patient
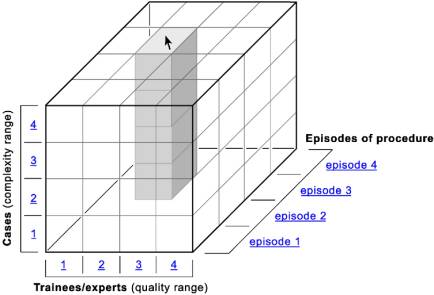
Figure 8. Selecting a particular intervention episode across all patients for one particular trainee
The rational for supporting new-coming surgeons to navigate through the case/trainee/phase library is that we apprehend learning as the saturation of all possible combinations of situations. The cells (cubettes) contain the VR episodes and allow new trainees to observe medical interventions and add alternative episodes created for other patients or make new episodes by themselves. The DIME project intends to implement and evaluate the effectiveness of this navigational mechanism and generalize it into architecture for medical training at a more global scale.
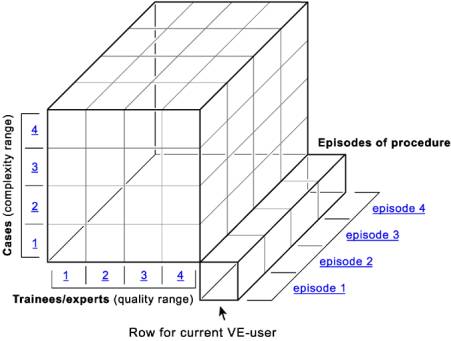
Figure 9. Single big cube and VE-user row (shopping mode)
In this mode the VE-user is studying the procedure for a specific case while having access to the reference cube. The case under study is presented without annotations; the reference cube contains only different cases. The user can practice and make his/her own solutions and annotations or sample solutions and annotations found in the reference cube. If the user feels that a mistake is made, he/she can step back through the episodes to make corrections.

Figure 10. The VE-user row only (operation room mode)
Here, the trainer can evaluate the progress made by the trainee. In the final situation we expect the entire surgical training curriculum to consist of multiple big cubes and episode-collection row (mega store mode). Each of the cubes is then a treatment category like inserting the AAA endograft stent, the stitching in the Lichtenstein method, etc.
Conclusion
Though virtual reality is one of the prime candidates in vitalizing learning by its realism and direct appeal to the students' natural affordance to act upon urgencies rather than to "know" what experts are saying; VR in itself is not enough to make the learning more effective. Obviously, the realism in VR cannot exceed the real situation itself. As the experiences with Link Trainers for airplane pilots has shown, we know that the simulation can be more effective, once it elicits the novice to go into critically complex situations; exactly those situations that we never hope to meet in reality. The added value is not just that the learner's reflexes are trained to survive in the panic of preciously decisive seconds. The value is also that learners can best understand the fundaments of complex mechanisms when they are forced to work on the edge of what is a success versus a failure. Training through real-patient interventions are not allowed to approach this area. That is why the VR-based medical intervention is an even better preparation to the first clinical steps compared to witnessing dozens of impeccable operations performed by the master.
This paper showed: the need for an adequate, more articulated learning paradigm like constructivism, but also the need for additional background processes during the execution of VR in learning situations. Most important is that there is a continuum between the literal recordings of video and voice-over of real surgical actions and the vectorized model of how meaningful parameters describe and predict the critical effects, for instance the morphological, textural and hydro-mechanical processes of blood in the stented aorta. But VR also provides the scaffolding of learning of the complete vascular intervention with complementary surgical skills such as endoscopy, micro-venereal stitching, and reinforcing the mechanical functions of the abdominal regions as in the Liechtenstein methods.
VR-based training systems are urgently-needed in developing countries and will stimulate the innovation and spread of expertise among countries in the world. The idea of Virtuality is clear: Let best practice be demonstrated on the WWW so that medical doctors in remote areas may witness the more advanced approaches without any delay and make them aware of how better intervention methods (not necessarily more expensive) can be applied in their own situations. The same perspective holds for the transfer of agricultural, technical and social skills: VR allows the observation of top-performances and let the newly emerging experts try out its repercussions before the real patient or machinery is needed.
References
Beck K. and Cunningham W. (1989). A laboratory for teaching object-oriented thinking. In Proc. OOPSLA'89, ACM Sigplan Notices 17(4), pp. 1-6.
Brown, Ann (1994). The advancement of learning. In Collins, A., Brown, J. S., & Newman, S. E. (1989); Educational Researcher, 23, 8, 4 12 Nov.
Collins, A., Brown, J. S., & Newman, S. E. (1989). Cognitive apprenticeship: Teaching the crafts of reading, writing, and mathematics. In L. B. Resnick (Ed.), Knowing, learning, and instruction: Essays in honor of Robert Glaser (pp. 453-494). Hillsdale, NJ: Lawrence Erlbaum Associates.
Kommers, P.A.M & Zhiming, Z.. (1998). Conceptual Support with Virtual Reality in Web-based Learning. International Journal of Continuing Engineering Education and Life-Long Learning, 8, No 1/2.,184-204.
Kommers, P.A.M. (2003). Experiential learning through constructivist learning tools. International Journal of Computers and Applications, 25, 1, 1-12
Lanier, Jaron; (1992). Virtual reality: The promise of the future. Interactive Learning International, 8, 4, 275-79.
McLellan, Hilary (1995). Magical stories: Blending virtual reality and artificial intelligence Imagery and Visual Literacy: Selected Readings from the Annual Conference of the International Visual Literacy Association Tempe, Arizona, October 12- 16, 1994.
Moshell, J.M., and Hughes, C.E. (1994). Shared virtual worlds for education. Virtual Reality World, 2, 1, 63-74.
Psotka, Joseph (1`995). Immersive training systems: Virtual reality and education and training. Instructional Science, 23, 5-6, 405-31.
Author Biographical Sketches
All authors are members of the DIME project; intended to integrate virtual reality model and interaction procedures in medical training, especially in vascular surgery. Piet Kommers is senior lecturer at Twente University and honorary professor at the UNESCO International Research and Training Centre in Kiev. Steffan Rödel is assistant surgeon in the Medical Hospital "Spectrum" in Enschede. Jan-Maarten Luursema is PhD student in the Faculty of behavioral Sciences in the University of Twente and specializes in VR for Training purposes. Bob Geelkerken is surgeon in the "Spectrum" hospital and Eelco Kunst is designer and director of Kunst & van Leerdam Medical Technology in Enschede, the Netherlands as well.
|
Dr. Piet KommersFaculty of Behavioral Sciences University of Twente P.O. Box 217 7500 AE Enschede The Netherlands Tel. +31 53 4893576 or 3611 Fax +31 53 4894580 |
|

Dr. Piet Kommers is Assistant Professor in the Faculty of Educational Science and Technology at Twente University in the Netherlands. His research field is the design and application of media in learning situations. His courses are Multimedia Design, Virtual Reality and Societal Effects of ICT. Concept mapping and metaphoric design stages play an important role here. Projects are undertaken in the field of Virtual Reality for Learning and Multicultural Communication. The learning processes at individual and societal levels manifest in terms of existential expressions and awareness. Media play an ever more important role in it.
Conceptual representations for meta-cognitive awareness become a default language for identity and road maps for changing oneself. The high saturation of communication infrastructure offers the opportunity to participate in learning communities. Sharing experience and finding the right sparring partners for exploring alternative approaches in one's job and continuous learning becomes realistic and offers a more dynamic personal development.
Schools, Professional Training and Human Resource Management face the challenge to include and build upon personal growth and attitudes. The priority in learning is not restricted to the access and assimilation of knowledge and skills. Finding ways to convey one's own further learning is priority number one. The WWW, adjacent to the face-to-face communication, is a valuable support facility. The art of designing WWW-based facilities and procedures is keen on both the nature and culture of the human mind. We may expect that education in the new era will have less and less to do with the transfer of knowledge on the shelf; the key issue is to facilitate the new learning modalities of the younger generation. We can hardly fall back on proven methodologies if it comes to media design`. In a certain way it is a self-organizing process where prior goals undergo evolution continuously. As new media appear daily, it is vital that those who are responsible for learning, communication and cooperation are willing to play with its potential; they will soon discover that a sense of pragmatism helps to attain the higher missions as well.